







Rakesh Jain, MD, MPH
Clinical Professor
Department of Psychiatry
Texas Tech Health Sciences Center, School of Medicine
Midland, Texas
Recent Evidence for Treatment Augmentation
With Second-Generation Antipsychotics
in Major Depressive Disorder
Supported by an educational grant from Otsuka and Lundbeck Alliance

●Please feel free to use, update, and share some or all of these slides in your noncommercial presentations to colleagues or patients
●When using our slides, please retain the source attribution:
●These slides may not be published, posted online, or used in commercial presentations without permission. Please contact permissions@clinicaloptions.com for details
About These Slides


Slide credit: clinicaloptions.com
Loading…

Disclosures
The faculty reported the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME/CE activity:
Rakesh Jain, MD, MPH, has disclosed that he has received consulting fees from Acadia, Alfasigma, Alkermes, Allergan, Eisai, Evidera, Impel, Janssen, Lilly, Lundbeck, Merck, Neos Therapeutics, Neurocrine, Osmotica, Otsuka, Pamlab, Pfizer, Shire, Sunovion, Supernus, Takeda, and Teva; has received fees for non-CME services from Alkermes, Allergan, Ironshore, Janssen, Lilly, Lundbeck, Merck, Neos Therapeutics, Neurocrine, Otsuka, Pamlab, Pfizer, Shire, Sunovion, Takeda, Teva, and Tris; has received funds for research support from Allergan, Lilly, Lundbeck, Otsuka, Pfizer, Shire, and Takeda; and that his spouse/partner has received consulting fees from Lilly, Otsuka, Pamlab, and Sunovion and fees for non-CME services from Lilly.

Partial Response and Nonresponse to Antidepressant Treatment
Partial Response
(or Response)
●Improvement of symptoms
●≥ 50% decrease in HAM‐D or MADRS
Relapse
●Return of symptoms after remission
Recurrence
●Return of symptoms after recovery
McIntyre. Clin Ther. 2006;28:1882. Zimmerman. J Psychiatr Res. 2004;38:577.
Saltiel. Neuropsychiatr Dis Treat. 2015;11:875. Lenox-Smith. J Affect Disord. 2014;169:149.
Remission
●Return to “wellness” or disappearance of symptoms
●Most frequently measured as HAM‐D ≤ 7 or MADRS ≤ 10
Recovery
●Remission for ≥ 2 mos


Slide credit: clinicaloptions.com







“Normalcy”
Symptoms
Syndrome
Remission
Response
Relapse
Recovery
Recurrence
Relapse/
recurrence
Remission/recovery
Relapse/
recurrence




First episode
Second episode
Third episode
Loading…

When MDD Treatment Fails
●In 30% to 45% of patients, remission is not achieved
with a single antidepressant, even at adequate dosage
and period[1]
‒Antidepressant efficacy decreases with successive trials[2]
‒More than 2 failed trials: treatment-resistant depression


Slide credit: clinicaloptions.com
1. Fava. J Clin Psychiatry. 2000;61 Suppl 1:26. 2. Rush. Am J Psychiatry. 2006;163:1905. 3. Russell. J Clin Psychiatry. 2004;65:341.
30%
70%



Level 4: Consider
●MAOI augmentation
(AVOID CONTRAINDICATED COMBINATIONS)
●FL-methylfolate triple drug combinations*
SSRI/ SNRI + mirtazapine + bupropion
SSRI/SNRI + mirtazapine + lithium
SSRI/SNRI + bupropion + second- generation antipsychotic
*Little evidence to support/refute this approach
MDD Treatment Augmentation: Florida Best Practice Psychotherapeutic Medication Guidelines

Level 1: Monotherapy
SSRI
SNRI
Vortioxetine
Bupropion
Mirtazapine

Level 2: Add
●Evidence-based psychotherapy
●Second-generation antipsychotic FDA-approved as adjunctive treatment for MDD
●Intranasal esketamine or intravenous racemic ketamine
●Another antidepressant (do not combine SSRI and SNRI)

Level 3: SSRI/SNRI +
●Lithium
●T3
●L-methylfolate
●S-adenosylmethionine
●Quetiapine (tolerability concerns)


Slide credit: clinicaloptions.com
●McIntyre. J Clin Psychiatry 2017;78:703.

MDD Treatment Augmentation:
Second-Generation Antipsychotics
1. Aripiprazole PI. 2. Olanzapine/fluoxetine PI. 3. Quetiapine XR PI. 4. Brexpiprazole PI.
Agent
FDA Approval for MDD Treatment Augmentation
Aripiprazole[1]
2007
Olanzapine/ fluoxetine[2]
2009
Quetiapine XR[3]
2009
Brexpiprazole[4]
2015


Slide credit: clinicaloptions.com
Agent
FDA Approval for MDD Treatment Augmentation
Asenapine
No
Clozapine
No
Cariprazine
No
Iloperidone
No
Lumateperone
No
Lurasidone
No
Paliperidone
No
Risperidone
No
Sulpiride
No
Ziprasidone
No



MDD Treatment Augmentation With
Second-Generation Antipsychotics: Considerations
Efficacy
●Best studied strategy, good efficacy[1]
●FDA approved options
●Included in guideline recommendations[2]
Tolerability (varies by agent)[3]
●Neuroendocrine
‒Prolactin
●Metabolic
‒Weight, lipids, glucose regulation
●Extrapyramidal symptoms
‒Tardive dyskinesia, neuroleptic malignant syndrome, akathisia, parkinsonism, dystonic reactions
1. Papakostas. J Clin Psychiatry. 2009;70 Suppl 6:16. 2. McIntyre. J Clin Psychiatry 2017;78:703.
3. Keepers. APA Practice Guideline. 2020. https://www.psychiatry.org/psychiatrists/practice/clinical-practice-guidelines.


Slide credit: clinicaloptions.com

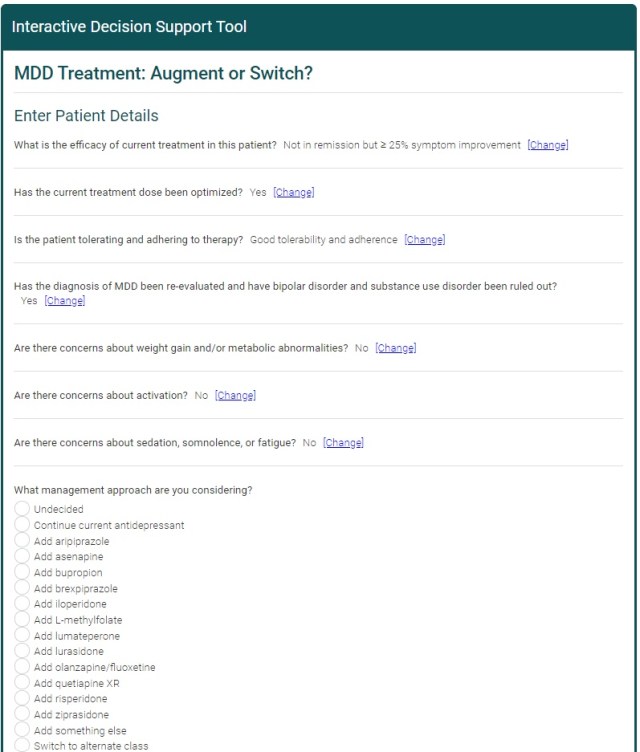
CCO Online Interactive Treatment Decision Support Tool for MDD Treatment
●Enter specific patient characteristics and get recommendations from a panel of 5 experts
‒Leslie Citrome, MD, MPH
‒Christoph U. Correll, MD
‒Rakesh Jain, MD, MPH
‒Roger McIntyre, MD, FRCPC
‒Michael E. Thase, MD


Slide credit: clinicaloptions.com
Available at clinicaloptions.com/AdvancingMDDTreatment

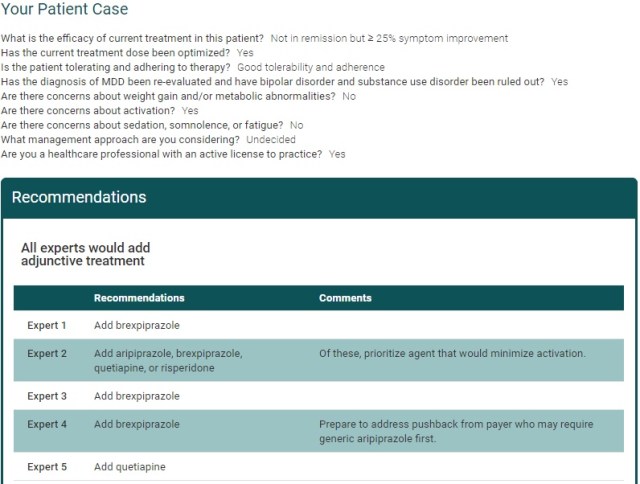
Expert Recommendations for Case: Patient Not in Remission but ≥ 25% Symptom Improvement


Slide credit: clinicaloptions.com

Loading…


Khullar 2006
Mattingly 2006
McIntyre 2006
Earley 2007
El-Khalili 2008
MDD Treatment Augmentation With
Second-Generation Antipsychotics: 2009 Meta-Analysis
●Meta-analysis of 16 randomized, placebo-controlled trials of adjunctive second-generation antipsychotics in patients with treatment-resistant major depressive disorder (N = 3480)


Slide credit: clinicaloptions.com
Nelson. Am J Psychiatry. 2009;166:980.
Test for overall effect

Response Rate
Fixed OR (95% CI) P Value
1.39 (1.05-1.84) .02
1.83 (1.18-2.82) .007
1.60 (1.24-2.08) .0004

Thase 2006
Shelton 2001
Shelton 2005
Corya 2006
Thase II 2006
2.07 (1.58-2.72) < .00001
1.69 (1.46-1.95) .00001

Berman 2007
Marcus 2008
Berman 2008

Mahmoud 2007
Keitner 2009
Reeves 2008

Subtotal
Subtotal
Subtotal
Subtotal





0.5

1

2

5

10
Favors Control
Favors Treatment


Treatment, N
Control, N
181
185
174
540
172
184
169
525
8
24
29
327
289
677
7
13
29
160
143
352
137
62
12
211
131
33
11
175
10
146
230
102
98
586
10
142
56
104
102
414
2014
1466
All agents:
●More effective than placebo
‒No differences in ORs among agents
●Had higher rates of discontinuation for adverse events than did placebo
Quetiapine
Risperidone
Olanzapine
Aripiprazole

Quetiapine XR (250-400 mg)
1.85
(0.19 to 7.14)
1.85
(0.79 to 3.57)
0.99
(0.36 to 4.00)
1.45
(0.42 to 9.09)
1.54
(0.57 to 6.25)
5.68
(1.38 to 90.42)
6.40
(2.94 to 17.83)
-0.03
(-0.49 to 0.38)
Risperidone
0.57
(0.18 to 3.62)
0.30
(0.09 to 2.05)
0.73
(0.22 to 4.78)
0.52
(0.16 to 3.47)
2.10
(0.47 to 43.16)
2.37
(0.87 to 11.14)
-0.06
(-0.34 to 0.19)
-0.04
(-0.45 to 0.41)
Quetiapine XR (150-250 mg)
1.09
(0.12 to 1.42)
0.85
(0.25 to 5.26)
0.90
(0.34 to 3.57)
3.32
(0.81 to 52.63)
3.73
(1.77 to 10.13)
-0.12
(-0.48 to 0.16)
-0.10
(-0.51 to 0.29)
-0.06
(-0.40 to 0.22)
Aripiprazole (Standard)
0.51
(0.12 to 1.42)
0.87
(0.22 to 2.36)
7.59
(0.60 to 37.02)
2.72
(1.34 to 6.82)
-0.16
(-0.59 to 0.17)
-0.14
(-0.60 to 0.29)
-0.10
(-0.51 to 0.24)
-0.04
(-0.34 to 0.24)
Aripiprazole (Low)
1.25
(0.21 to 4.26)
10.26
(0.58 to 53.19)
2.88
(1.00 to 12.96)
-0.16
(-0.51 to 0.13)
-0.14
(-0.54 to 0.27)
-0.10
(-0.43 to 0.20)
-0.04
(-0.30 to 0.25)
0
(-0.32 to 0.36)
Olanzapine/
Fluoxetine (Standard)
8.53
(1.08 to 36.67)
3.52
(1.74 to 8.48)
-0.40
(-0.91 to 0.06)
-0.38
(-0.92 to 0.17)
-0.34
(-0.83 to 0.13)
-0.28
(-0.72 to 0.18)
-0.24
(-0.72 to 0.27)
-0.24
(-0.64 to 0.16)
Olanzapine/
Fluoxetine (Low)
0.43
(0.09 to 4.05)
-0.43
(-0.72 to -0.21)
-0.41
(-0.77 to -0.06)
-0.37
(-0.64 to -0.14)
-0.31
(-0.49 to -0.12)
-0.27
(-0.53 to 0.01)
-0.27
(-0.48 to -0.08)
-0.03
(-0.45 to 0.38)
Placebo
MDD Treatment Augmentation With
Second-Generation Antipsychotics: 2015 Meta-Analysis
●Meta-analysis of 18 randomized, placebo-controlled trials of adjunctive second-generation antipsychotics at standard and low doses in patients with treatment-resistant major depressive disorder (N = 4422)
Zhou. Int J Neuropsychopharmacol. 2015;18:pyv060.


Slide credit: clinicaloptions.com
Efficacy by Depression Symptom Score, standardized mean differences (95% CI)
Tolerability by OR of adverse event discontinuation (95% CI)
All standard-dose agents:
●More effective than placebo
●Had higher rates of discontinuation for adverse events than did placebo

MDD Treatment Augmentation With Second-Generation Antipsychotics: Efficacy by Degree of Resistance
●Meta-analysis of 11 randomized, controlled trials of adjunctive second-generation antipsychotics in patients with treatment-resistant MDD (N = 3341)
Wang. Int J Neuropsychopharmacol. 2015;18:pyv023.
●Improved efficacy with increasing rates of resistance


Slide credit: clinicaloptions.com
History of Treatment Failures:
Meta-Regression of Response Rate
0
2
2 to 4

Response, log of Risk Ratio



.2
.3
.4
.5
.6











MDD Treatment Augmentation: Key Studies of
Second-Generation Antipsychotics
1. Berman. J Clin Psychiatry. 2007;68:843. 2. Tohen. J Clin Psychiatry. 2010;71:451.
3. El-Khalili. Int J Neuropsychopharmacol. 2010;13:917. 4. Thase. J Clin Psychiatry. 2015;76:1224.
N
Mean Change in MADRS After 6 Wks
Agent
Comparator
MDD Population
Treatment
Comparator
Treatment
Comparator
P value
Aripiprazole + antidepressant[1]
Placebo
Incomplete response
184
178
-8.80
-5.80
< .001
Olanzapine/ fluoxetine[2]
Fluoxetine
Treatment resistant
462
342
-12.28
-8.48
< .001
Olanzapine/ fluoxetine[2]
Olanzapine
Treatment resistant
462
342
-12.28
-8.52
< .001
Quetiapine XR + antidepressant[3]
Placebo
Inadequate response
148*
148
-14.70*
-11.70
< .01
Brexpiprazole + antidepressant[4]
Placebo
Inadequate response
175
178
-8.36
-5.15
.0002


Slide credit: clinicaloptions.com


*300 mg/day.
All are superior to placebo, but none has been shown to be superior to others

MDD Treatment Augmentation With Aripiprazole
●Multicenter, randomized, double-blind, placebo-controlled phase III study in patients with MDD and incomplete response to antidepressant therapy (N = 362)
*
*
*
*
*
Wk
Berman. J Clin Psychiatry. 2007;68:843.


Slide credit: clinicaloptions.com
Placebo +
SSRI
(n = 172)
Aripiprazole +
SSRI
(n = 181)






0
-2
-4
-6
-8
-10
-12
-14
-16
Baseline
1
2
3
4
5
6










Mean Change
in MADRS Total Score
*P < .001

MDD Treatment Augmentation With Aripiprazole: Safety
Berman. J Clin Psychiatry. 2007;68:843.


Slide credit: clinicaloptions.com
Adverse Events, n (%)
Aripiprazole +
Antidepressant (n = 182)
Placebo +
Antidepressant (n = 176)
Any
149 (81.9)
110 (62.5)
Akathisia
42 (23.1)
8 (4.5)
Restlessness
26 (14.3)
6 (3.4)
Upper respiratory tract infection
15 (8.2)
7 (4.0)
Insomnia
14 (7.7)
4 (2.3)
Blurred vision
12 (6.6)
3 (1.7)
Fatigue
11 (6.0)
6 (3.4)
Headache
11 (6.0)
19 (10.8)
Diarrhea
6 (3.3)
10 (5.7)
Dry mouth
6 (3.3)
11 (6.3)
Nausea
5 (2.7)
9 (5.1)



Olanzapine/Fluoxetine in Treatment-Resistant MDD
Tohen. J Clin Psychiatry. 2010;71:451.


Slide credit: clinicaloptions.com
●Pooled analysis of 5 outpatient studies of olanzapine/fluoxetine in patients with treatment-resistant MDD (N = 1146)
*P < .001 vs fluoxetine
†P ≤ .011 vs olanzapine
*
*
*
*
*
*
Fluoxetine
(n = 203)
Olanzapine
(n = 197)
Olanzapine/fluoxetine
combination
(n = 198)
Wk



0
-2
-4
-6
-8
-10
-12
-14
-16
Baseline
1
2
3
4
5
6


















7
8
*
*
*
†
†
†
†
†
†

Mean Change
in MADRS Total Score










Olanzapine/Fluoxetine in Treatment Resistant MDD: Safety
Tohen. J Clin Psychiatry. 2010;71:451.


Slide credit: clinicaloptions.com
Adverse Events, %
Olanzapine/ Fluoxetine
(n = 462)
Fluoxetine
(n = 342)
Olanzapine
(n = 342)
P Values
Overall
Olanzapine/ Fluoxetine
vs Fluoxetine
Olanzapine/ Fluoxetine
vs Olanzapine
Increase weight
35.0
6.8
39.7
< .001
< .001
.353
Increased appetite
32.0
5.8
30.7
< .001
< .001
.829
Dry mouth
28.5
8.7
31.7
< .001
< .001
.514
Somnolence
17.5
5.3
12.1
< .001
< .001
.158
Fatigue
14.0
7.8
14.1
.070
.055
1.00
Headache
12.5
19.4
13.1
.103
.060
.882
Peripheral edema
12.0
1.0
7.5
< .001
< .001
.177
Hypersomnia
10.5
2.4
11.1
< .001
< .001
.873
Tremor
10.5
8.7
8.0
.686
.615
.490




MDD Treatment Augmentation With Quetiapine XR
●Multicenter, randomized, double-blind, placebo-controlled phase III study of in patients with MDD and incomplete response to antidepressant therapy (N = 446)
El-Khalali. Int J Neuropsychopharmacology. 2010;13:917.


Slide credit: clinicaloptions.com
†
‡
*
Wk



0
-2
-4
-6
-8
-10
-12
-14
-16
Baseline
1
2
3
4
5
6












†
†
†


Placebo + antidepressant
(n = 143)
Quetiapine XR
150 mg/day + antidepressant
(n = 143)
Quetiapine XR
300 mg/day + antidepressant
(n = 146)


Mean Change
in MADRS Total Score
*P < .05
†P < .01
‡P < .001
(all vs placebo)

MDD Treatment Augmentation With Quetiapine XR: Safety
El-Khalali. Int J Neuropsychopharmacology. 2010;13:917.


Slide credit: clinicaloptions.com
Adverse Events, n (%)
Quetiapine XR 150 mg +
Antidepressant (n = 148)
Quetiapine XR 300 mg +
Antidepressant (n = 149)
Placebo +
Antidepressant (n = 148)
Dry mouth
52 (35.1)
66 (44.3)
13 (8.8)
Somnolence
43 (29.1)
43 (28.9)
6 (4.1)
Sedation
25 (16.9)
33 (22.1)
6 (4.1)
Dizziness
17 (11.5)
21 (14.1)
8 (5.4)
Constipation
11 (7.4)
16 (10.7)
5 (3.4)
Nausea
13 (8.8)
15 (10.1)
12 (8.1)
Headache/fatigue
16 (10.8)/23 (15.5)
11 (7.4)/10 (6.7)
20 (13.5)/7 (4.7)
Diarrhea
10 (6.8)
10 (6.7)
10 (6.8)
Increased appetite
8 (5.4)
10 (6.7)
8 (5.4)
Increased weight
3 (2.0)
9 (6.0)
1 (0.7)
Irritability
9 (6.1)
5 (3.4)
9 (6.1)
Insomnia
16 (10.8)
12 (8.1)
10 (6.8)









*









†
‡


MDD Treatment Augmentation With Brexpiprazole
●Randomized, placebo-controlled phase III study of adjunctive brexpiprazole in patients with MDD and incomplete response to antidepressant therapy (N = 353)
Thase. J Clin Psychiatry. 2015;76:1224.


Slide credit: clinicaloptions.com

Mean (SE) Change
in MADRS Total Score
Wk





0
-2
-4
-6
-8
-10
-12
-14
-16
Baseline
1
2
3
4
5
6



‡
‡
Placebo +
antidepressant
(n = 178)
Brexpiprazole + antidepressant
(n = 175)

*P < .05
†P < .01
‡P < .001
(all vs placebo)

MDD Treatment Augmentation With Brexpiprazole: Safety
Thase. J Clin Psychiatry. 2015;76:1224.


Slide credit: clinicaloptions.com
Treatment-Related Adverse Events, n (%)
Brexpiprazole +
Antidepressant
(n = 188)
Placebo +
Antidepressant
(n = 191)
≥ 1 treatment-related adverse event
111 (59.0)
89 (46.6)
Serious adverse events
2 (1.1)
2 (1.0)
Discontinuation due to treatment-related adverse event
6 (3.2)
0
Treatment-related adverse event occurring in ≥ 5% of brexpiprazole group
●Weight gain
●Akathisia
15 (8.0)
14 (7.4)
6 (3.1)
2 (1.0)


*Odds ratios based on multivariable logistic regression with adherence as dependent variable.
Antipsychotics: Impact of AEs on Adherence
●Survey of N = 876 community-dwelling people with schizophrenia
DiBonaventura. BMC Psychiatry. 2012;12:20.


Slide credit: clinicaloptions.com
Likelihood of Complete Adherence

Agitation
Tremors
Restlessness/feeling jittery
Insomnia
Increased blood glucose levels
Weight gain
Painful menstrual periods
Gynecomastia and galactorrhea
Decreased interest in sex
Sexual dysfunction
Sedation
Difficulty thinking/concentrating
Sleepiness
Dizziness
Nausea/vomiting
Constipation
0
1.0
0.5
1.5
2.0
2.5
3.0
3.5

Adjusted Odds Ratios
Reduced Adherence





































EPS/agitation
OR: 0.57
Metabolic
OR: 0.64
Prolactin/endocrine
OR: 0.69
Sedation/cognition
OR: 0.70
Gastrointestinal
OR: 0.79
Adverse Event Clusters*

Reduced Adherence


Second-Generation Antipsychotics: Weight Gain Among Adults in Short-term Randomized Controlled Studies


Slide credit: clinicaloptions.com
Weight Gain ≥ 7% of Baseline
Medication[1]
Schizophrenia
Bipolar Mania
MDD
Bipolar Depression
Iloperidone
10
—
—
—
Asenapine
35
19
—
—
Lurasidone
67
—
—
58[2]
Brexpiprazole
17
—
52
—
Cariprazine (≤ 6 mg/day)
34
No difference
—
—
Aripiprazole
21
No difference
22
—
Olanzapine/fluoxetine
6
6
3
6[2,3]
Paliperidone
35
—
—
—
Quetiapine IR
6
8
—
16[2]
Quetiapine XR
22
20
29
16[2]
Risperidone (≤ 8 mg/day)
18
18
—
—
Ziprasidone
16
58
—
—
1. Citrome. Int J Clin Pract. 2015;69:1211. 2. Citrome. CNS Spectr. 2014;19(suppl 1):4. 3. Citrome. Expert Opin Pharmacother. 2011;12:2751.

Second-Generation Antipsychotics: Metabolic AEs
●Systematic review and network analysis of 100 randomized, controlled trials
of 18 antipsychotics in schizophrenia (N = 25,952)
Subset of Agents FDA Approved in MDD Augmentation
P-Score Ranking of AEs From 0 to 1*
Weight Increase
Glucose
Increase
LDL-C
Increase
Total C
Increase
HDL-C Decrease
TG
Increase
Aripiprazole
.26
.55
.48
.50
.26
.33
Brexpiprazole
.45
.40
.66
.52
.18
.23
Quetiapine XR
.65
.47
.91
.82
.59
.71
Olanzapine/fluoxetine
.92
.67
.96
.91
.76
.83
Pillinger. Lancet Psychiatry. 2020;7:64.


Slide credit: clinicaloptions.com






*P-score ≥ .50 shown in red.

Antipsychotic-Associated Weight Gain:
Pharmacologic Interventions
●Meta-analysis of 32 randomized, controlled trials of 15 different medications (N = 1482)

Weighted Mean Difference in Bodyweight Change, kg (95% CI)

Favors Placebo

Favors Intervention
4

2

0


-2

6

-4


-6


Metformin + Sibutramine














Famotidine

Dextroamphetamine

Fluoxetine

Rosiglitazone

Orlistat

Nizatidine

Amantadine

Reboxetine

Topiramate

Sibutramine

D-Fenfluramine

Metformin
Maayan. Neuropsychopharmacology. 2010;35:1520.


Slide credit: clinicaloptions.com
Significant difference vs placebo




AEs: Medical Risk Prevention Strategies
At Treatment Initiation
(Primary Prevention)
●Healthy lifestyle counseling/intervention
●Start with lower-risk antipsychotic


Slide credit: clinicaloptions.com
Correll. CNS Spectr. 2007;12:12.
If AE is Present
(Secondary Prevention)
●Healthy lifestyle counseling/intervention
●Consider changing to lower-risk antipsychotic
●Consider weight loss intervention
If AE Progresses/Serious
(Tertiary Prevention)
●Healthy lifestyle counseling/intervention
●Consider changing to lower-risk antipsychotic
●Add targeted treatment for pathological values
●Consider referral to specialist






Algorithm to Manage Treatment-Emergent Akathisia
Salem. Current Neuropharmacol. 2017;15:789.


Slide credit: clinicaloptions.com

Reduce dose

Change
antipsychotic

Switch to low
potency first-generation
antipsychotic

Switch to second-generation
antipsychotic with
lower akathisia potential
(eg, quetiapine)

Add antiakathisia
agent








First line

Second line

Switch to clozapine

Beta-blockers:
Propranolol
(40-80 mg/day)

5-HT2A antagonist:
Mirtazapine (15 mg/day)

Anticholinergics (mainly with parkinsonism):
Biperiden (2-6 mg/day)
Benztropine (1.5-8 mg/day)
Trihexyphenidyl (2-10 mg/day)

Amantadine (100 mg/day)
Clonidine (up to 0.15 mg/day)

Benzodiazepines:
Lorazepam (1-2 mg/day)
Clonazepam (0.5-1 mg/day)
Diazepam (5-15 mg/day)

5-HT2A antagonist:
Mianserin (up to 0.15 mg/day)
Cyproheptadine (8-16 mg/day)
Akathisia in schizophrenia and mood disorders








My approach in MDD augmentation:
avoid unapproved antipsychotics
Loading…

Expert Recommendations for Treatment Augmentation:
Activation/Akathisia Concerns


Slide credit: clinicaloptions.com

Second-Generation Antipsychotics: Sexual AEs
1. Kristensen E. Dan Med Bull. 2002;49:349. 2. Fava. Prim Care Companion CNS Disord. 2011;13:PCC.10m00994. 3. Pillinger. Lancet Psychiatry. 2020;7:64. 4. Brexpiprazole Prescribing Information.


Slide credit: clinicaloptions.com
Symbols: ↓ = inhibits/reduces; ↑ = promotes/increases.
●Review based on few systemic studies[1]
●Aripiprazole, brexpiprazole also associated with sedation and weight gain,
but no evidence of sexual dysfunction in registration trials[2-4]
Antipsychotic Agent
Libido/Arousal
Orgasm
Sedation
Weight
Other
Clozapine
↓↓
↓
↑↑↑
↑↑↑
Priapism
Olanzapine
↓
↓
↑
↑↑↑
Priapism
Risperidone
↓
↓
↑
↑
Priapism
Ziprasidone
↓
↓
↑
(↑)
Sulpiride
↓↓
↓
↑
↑
Quetiapine
↓
↓
↑↑
↑

Algorithm to Manage Treatment-Emergent
Sexual Dysfunction
Clayton. Psychiatr Clin North Am. 2016;39:427.

Patient warrants
treatment with
antipsychotic

Patient already
has SD or is
concerned about
developing SD?

Choose a
medication with a
more favorable
SD profile

Choose any
appropriate
medication and
monitor for SD

Patient develops
sexual AE

Patient and
physician amenable
to regimen change?

•Watch and wait
•Reduce dose
•Drug holiday
•Nonpharmacologic
options

Is the current regimen
fully effective for the
primary psychiatric
target symptoms?

Add an antidote to
current regimen

Change to a
medication known
to cause fewer
sexual AEs









YES
NO
YES
NO
YES
NO


Slide credit: clinicaloptions.com

Clinical Manifestations of Hyperprolactinemia
●Anxiety, depression, hostility
●Decreased bone mineral density and osteoporosis
●Infertility
●Disturbed menstrual cycles
●Anovulation, amenorrhea, or irregular cycles
●Decreased testosterone levels and sperm mobility
●Sexual dysfunction
‒Decreased libido/arousal;
un- or hypo-orgasmia
●Increased risk of cardiovascular disorders
●Breast engorgement and galactorrhea
●Increased risk of breast cancer
●Increased risk of tardive dyskinesia?
●Abnormal function of the immune system?
Halbreich. Psychoneuroendocrinology. 2003;28:53.


Slide credit: clinicaloptions.com

Variation in Antipsychotics: Effect on Prolactin Increase
●Meta-analysis of 212 studies of patients with schizophrenia (N = 43,049 )[1]
●Brexpiprazole, not shown, does not generally increase prolactin levels[2]
1. Leucht. Lancet. 2013;382:951. 2. Ivkovic. J Clin Psychopharmacol. 2019;39:13.


Slide credit: clinicaloptions.com

Prolactin Increase, Standardized Mean Difference (95% Cl)

Aripiprazole -0.22 (-0.46 to 0.03)
Quetiapine -0.05 (-0.23 to 0.13)
Asenapine 0.12 (-0.12 to 0.37)
Olanzapine 0.14 (0 to 0.28)
Chlorpromazine 0.16 (-0.48 to 0.8)
Iloperidone 0.21 (-0.09 to 0.51)
Ziprasidone 0.25 (0.01 to 0.49)
Lurasidone 0.34 (0.11 to 0.57)
Sertindole 0.45 (0.16 to 0.74)
Halperidol 0.70 (0.56 to 0.85)
Risperidone 1.23 1.06 to 1.40)
Paliperidone 1.30 (1.08 to 1.51)
0
1.0
-0.5
1.5
0.5

More Prolactin Increase
With Placebo














More Prolactin Increase
With Active Drug

MDD Treatment Augmentation With Second-Generation Antipsychotics: Managing Adverse Events
●Consider potential advantages and disadvantages for individual patients before prescribing
McIntyre. J Clin Psychiatry 2017;78:703.
American Psychiatric Association, Practice Guideline for the Treatment of Patients with Major Depressive Disorder; 2010.


Slide credit: clinicaloptions.com
●Dosing in MDD (in combination with antidepressants) is typically lower than in bipolar disorder and psychosis
‒Lower dose may minimize risk of adverse events
●Monitor:
‒Adverse events, including sedation, weight gain, akathisia and extrapyramidal symptoms
‒Weight, body mass index, and metabolic indices at baseline and regular intervals

Summary
●Goal of treating major depression remains full symptomatic and functional remission and recovery
●4 second-generation antipsychotics are approved by the FDA for use as antidepressant augmentation
‒All have demonstrated efficacy
●Adverse events often manageable with short- and long-term vigilance
‒Weight gain, hyperprolactinemia, sexual dysfunction, tardive dyskinesia, are among the issues to monitor


Slide credit: clinicaloptions.com




clinicaloptions.com/internalmedicine
Go Online for More CCO
Coverage of Depression!
CME-certified activities with expert faculty commentary
Additional unlocked slidesets with key information
Interactive Decision Support Tool on when to augment or switch MDD treatment











